
PCOS Phenotypes Explained: Why No Two Stories Are Alike
- Jessica Elliott
- Jan 14
- 4 min read
One of the most frustrating parts of living with PCOS is hearing conflicting information. One person struggles with weight and insulin resistance. Another has irregular periods but no metabolic concerns. Someone else was diagnosed only after fertility challenges.
All of these experiences can be PCOS.
PCOS is not a single presentation. It is a spectrum. Understanding PCOS phenotypes can help explain why symptoms vary so widely and why comparison often leads to confusion, self-doubt, and shame.
This matters not just medically, but emotionally and relationally as well.
What Are PCOS Phenotypes?
PCOS phenotypes are categories used to describe how polycystic ovary syndrome shows up in the body. They are based on the Rotterdam Criteria, which looks at three core features:
Irregular or absent ovulation
Clinical or biochemical signs of high androgens
Polycystic appearing ovaries on ultrasound
A diagnosis requires at least two of these three. The combination determines the phenotype.
There are four recognized phenotypes labeled A through D.
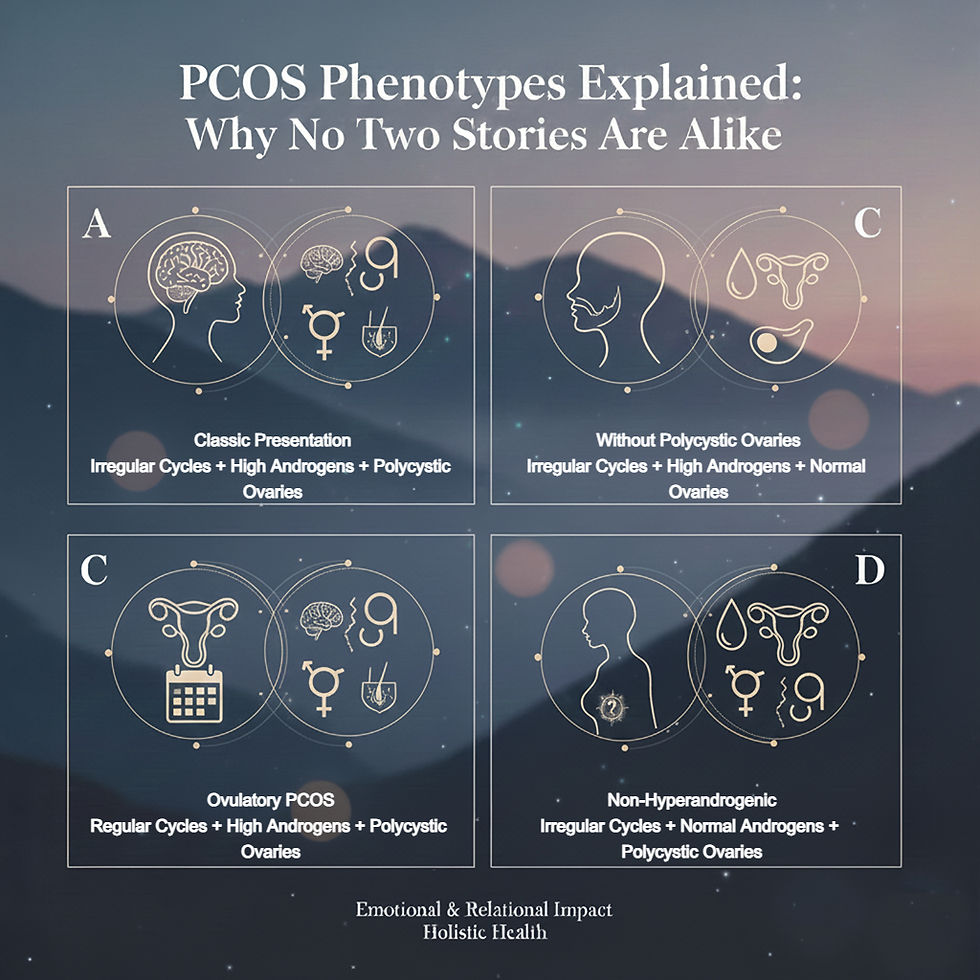
Phenotype A: The “Classic” PCOS Presentation
Phenotype A includes all three diagnostic features.
Irregular or absent periods
Elevated androgens such as testosterone
Polycystic ovaries
This phenotype is often what people think of when they hear PCOS.
Common experiences include weight changes, insulin resistance, acne, facial or body hair growth, scalp hair thinning, and fertility challenges. Emotionally, many individuals report feeling betrayed by their body, frustrated with medical care, or overwhelmed by managing multiple symptoms at once.
Mental health concerns such as anxiety, depression, and body image distress are common here, especially when symptoms are visible or misunderstood by others.
Phenotype B: PCOS Without Polycystic Ovaries
Phenotype B includes:
Irregular or absent ovulation
Elevated androgens
Normal appearing ovaries
This phenotype is often overlooked because ultrasounds do not show cystic ovaries. Individuals may be dismissed or told their labs are “not that bad.”
Symptoms often center around hormonal imbalance such as acne, hair changes, mood swings, and cycle irregularity. The emotional impact often comes from not being believed or feeling invalidated by providers or loved ones.
Many people with Phenotype B internalize the message that they are “not sick enough,” which can delay care and increase self-doubt.
Phenotype C: Ovulatory PCOS
Phenotype C includes:
Elevated androgens
Polycystic ovaries
Regular ovulation
This is sometimes called ovulatory PCOS and is one of the most confusing presentations.
People may have regular cycles and even conceive without assistance, yet still struggle with acne, hair growth, hair loss, or metabolic symptoms. Because periods appear “normal,” PCOS is often missed entirely.
Emotionally, this phenotype can create confusion and imposter syndrome. Individuals may minimize their struggles or feel guilty seeking support because they do not match the stereotypical PCOS narrative.
Phenotype D: Non Hyperandrogenic PCOS
Phenotype D includes:
Irregular or absent ovulation
Polycystic ovaries
Normal androgen levels
This phenotype lacks the visible androgen related symptoms often associated with PCOS. There may be fewer outward signs, but significant internal disruption.
People with Phenotype D may experience irregular cycles, infertility, fatigue, and metabolic changes without acne or excess hair growth. Because symptoms are less visible, emotional distress often centers around confusion, delayed diagnosis, and grief related to fertility or cycle unpredictability.
This phenotype highlights that PCOS is not always something you can see.
Why Phenotypes Matter for Mental Health
Understanding phenotypes helps dismantle comparison. It explains why one person’s PCOS looks different from another’s and why advice that helps one individual may not help another.
From a mental health perspective, phenotypes can validate experiences such as:
Feeling dismissed because symptoms do not fit the stereotype
Feeling ashamed because symptoms are visible
Feeling isolated when others with PCOS seem to have an easier path
Feeling disconnected from your body due to unpredictability
For couples, phenotype differences can also impact communication. One partner may struggle with visible symptoms affecting self-esteem, while another may be navigating fertility grief or medical burnout. Without context, these experiences can be misunderstood as overreactions rather than legitimate responses to chronic stress.
Moving Away from Comparison and Toward Compassion
No phenotype is “better” or “easier.” Each comes with its own challenges, risks, and emotional load.
When individuals understand their phenotype, they often experience relief. Not because it fixes everything, but because it offers language, validation, and direction.
PCOS is not a competition of symptoms. It is a complex condition that affects hormones, metabolism, mental health, identity, and relationships in deeply personal ways.
Your story does not need to look like anyone else’s to be real.
A Gentle Reminder
If you have PCOS and feel like your experience does not fit the narrative you see online, you are not broken and you are not alone. Your phenotype matters. Your symptoms matter. And your emotional experience deserves care and support.
Disclaimer:
This blog is for educational and informational purposes only and is not a substitute for medical or mental health care. PCOS presents differently in each individual. Please consult with a qualified medical provider or licensed mental health professional for personalized assessment and treatment.



Comments